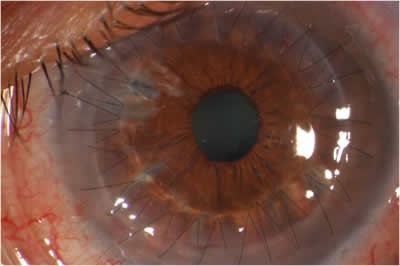
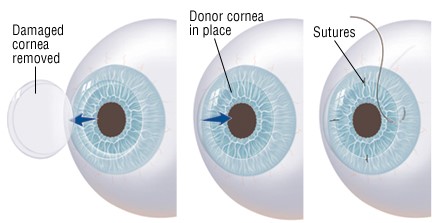
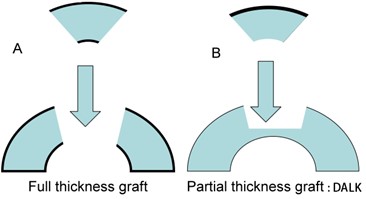
The full-thickness corneal transplant, or Penetrating Keratoplasty (PK), originated over 100 years ago. The procedure involves the transplantation of donor corneal tissue to replace the patient’s pre-existing, damaged central cornea. Usually, we remove the centra 7.5mm. This procedure is referred to as a full-thickness transplant because the entire damaged cornea is replaced by the donor cornea. There are a variety of conditions that can result in the need for a PK, including corneal swelling, scarring or distortion. These conditions blur the vision and may result from genetic conditions, infection or trauma.
Corneal transplantation, when indicated, can help to restore functional vision in an eye with corneal damage. However, like all surgeries, there is a risk that must be balanced against the degree of difficulty the patient is experiencing as a result of his or her corneal disorder. The most common threat to the success of a corneal transplant is graft rejection. Rejection occurs in about 10% of cases, but if risk factors are present the rate of rejection may be much higher for some individuals. In most instances, episodes of rejection can be controlled by topical steroid eye drops or other forms of medicine; however, rejection may result in a permanent swelling of the donor cornea causing blurred vision, leading to the need for another full-thickness transplant. Sutures are used to hold the donor corneal tissue in place during the recovery period. Occasionally, the sutures can become loose, which may result in infection or induce astigmatism. It is impossible to predict the glasses prescription that will result after a corneal transplant. It is common for a significant amount of farsightedness, nearsightedness or astigmatism to be present following a full-thickness cornea transplant. In some cases, the glass prescription is strong enough that eyeglasses alone cannot offer adequate vision or balance with the other eye. For these individuals, contact lenses or additional surgery may help to bring the eyes into focus and balance.
Full-thickness transplants are vulnerable to a traumatic injury that may result in rupturing the eye (even years after the original transplant) because the transplant never heals as strong as a normal cornea. Therefore, extra caution and some restrictions are required for life after undergoing corneal transplantation, which must be considered prior to surgery. Typically, the visual recovery time following a full-thickness transplant is 2 years. Patients who undergo full-thickness corneal transplants may be on an eye drop regimen usually forever, following surgery.
Till a few years ago we were using a sharp curved metal blade called a “trephine” to cut the cornea.
Today we use a Femtosecond laser. This is called LACT, laser-assisted corneal transplant.